
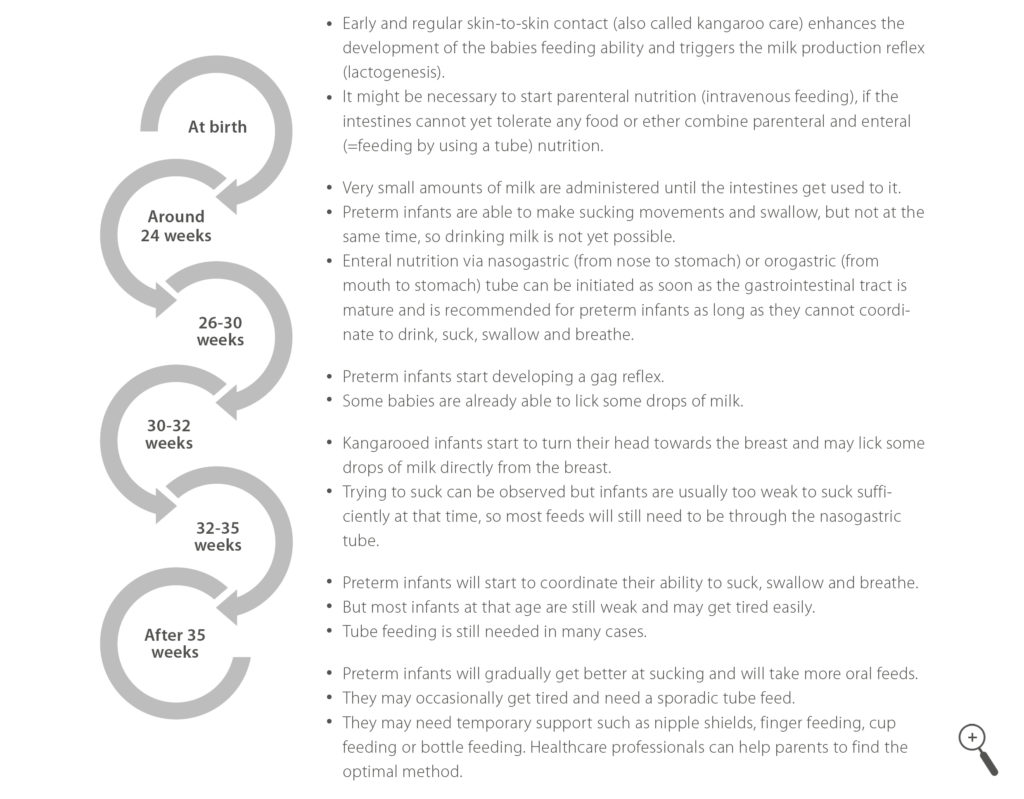
Feeding stages
The aim of nutritional support for a preterm baby is to achieve a similar growth rate compared to the foetus at the same age. In order to reach the optimal development experts recommend to start feeding as soon as possible after birth. However, it may not always be possible to start full feeding immediately after birth.
Enteral nutrition
means feeding the baby by using a nasogastric (via nose to stomach) or orogastric (via mouth to stomach) tube. It can be initiated as soon as the gastrointestinal tract is mature. This solution is recommended by most guidelines for preterm infants as long as they cannot coordinate to drink, suck, swallow and breathe. The ability for suck-feeding usually develops around 35 weeks of gestational age, so that infants born before 35 weeks will most likely require temporary tube feeding. During the first days of life, only very small amounts of milk are administered until the intestines get used to it.
The first steps towards breastfeeding can be initiated as soon as the condition of the preterm baby has stabilised. The learning process takes time and needs a lot of patience. The first step towards breastfeeding is kangaroo care which may already be commenced soon after birth. Health care professionals together with parents will decide if the preterm baby is stable enough for kangaroo care. Skin-to-skin contact will help the baby to develop the feeding abilities and also stimulates the milk production.
Around the age of 24 weeks, babies are able to do their first sucking movements but cannot coordinate sucking and swallowing yet.
Between 26 and 30 weeks the development progresses and babies will have a gag reflex, which helps to prevent choking. At this stage, some babies are already able to lick some drops of breast milk.
In the next two weeks, kangarooed infants will already start to turn their head towards the breast and may lick some drops of milk directly from the breast. But most feeds will still need to be through the nasogastric tube.
The ability to coordinate sucking, swallowing and breathing will be developed around the age of 35 weeks. But most infants at that age are still weak and may get tired easily. Hence, tube feeding is still needed in many cases.
The preterm infant will now get more active every day until even full breastfeeding is possible. Some hospitals work with so-called ‘early feeding scales’ for the assessment of feeding abilities or nutrition specialists check whether a preterm baby is ready to start oral feeding.
Babies may also need temporary support such as nipple shields, finger feeding, cup feeding or bottle feeding. There are numerous techniques for feeding a preterm baby with breast milk. Healthcare professionals or lactation specialists can help parents to find the optimal solution for them and their baby.
The EFCNI Academy offers an E-learning series on enteral preterm nutrition for junior to senior level healthcare professionals and medical specialists and nursing staff working in the field of paediatrics, neonatology or infant nutrition. Click HERE for more information.
What is parenteral nutrition?
Parenteral nutrition in preterm and ill babies is a feeding therapy that provides nutrition through the veins (into the bloodstream) to babies who cannot (yet) be adequately fed by mouth or through a feeding tube.
Preterm and ill babies are often fed through a tube that is passed through the mouth or the nose into the baby’s stomach or small intestine, usually on the first day of life. This so called enteral nutrition is used when the digestive tract is at least partly functioning, but the baby has sucking or swallowing difficulties due to immaturity, neuromuscular, heart, or other disorders. Through the tube, (fortified) human milk (breastmilk or donor milk) or formula can be given to the baby.
Today, one strives to provide at least minimal enteral nutrition from the first days of life, and therefore usually partial parenteral nutrition is provided combined with some enteral nutrition (fortified human milk or preterm formula).
Who needs parenteral nutrition, and why?
Most immature preterm babies need some parenteral nutrition during the first week of life because the amount of enteral nutrition that can be provided during the first days does not yet meet the nutrient needs. A sufficient supply of nutrients is necessary for brain development and in order to prevent the occurrence of nutrient deficits, which may result in growth failure. The duration for which parenteral nutrition is required depends on how quickly enteral nutrition is advanced and how soon the baby can tolerate full enteral feeding.
When is parenteral nutrition indicated?
If one expects that only limited amounts of enteral feeding with human milk or formula will be tolerated during the first week of life, parenteral nutrition is instituted shortly after birth to avoid starvation, preferably starting on the first day of life. Whenever possible, parenteral nutrition should be combined with some (even if minimal) enteral feedings and should be stepwise decreased as it is gradually replaced by increasing amounts of enteral nutrition as tolerated by the baby.
What is the composition of parenteral nutrition and how is it given to an infant?
Parenteral nutrition is a sterile (= clean and free from bacteria or other microorganisms) liquid form of nutrient supply. Its composition ensures that the baby’s energy and other nutrient requirements, which are age-related and influenced by illness and therapy, can be met. Parenteral nutrition preparations contain carbohydrates (the sugar glucose), amino acids (the building blocks of proteins), fats, salts (also called electrolytes), vitamins, minerals, trace elements, and water. The fluids are given into the bloodstream by placing a small needle or a tiny tube into a blood vessel in the baby’s hand, foot, scalp, navel, or elsewhere.
What are the benefits of parenteral nutrition?
Supplemental parenteral nutrition in addition to partial enteral nutrition supports a nutrient supply that can better match the baby’s needs when enteral nutrition tolerance is still limited or when sufficient enteral nutrition cannot be provided due to an underlying disease. Thereby, it may contribute to good postnatal growth and development.
What are the risks of parenteral nutrition?
Parenteral nutrition is often lifesaving for very preterm or very ill babies. However, parenteral nutrition is not without risk of complication. A common problem is the deficiency or excess of parenteral nutrition components. High glucose infusion, for example, can cause hyperglycaemia (“high blood sugar”) in the baby. Other risks include bloodstream infections, sepsis (“blood poisoning”), blood clots, and parenteral nutrition-associated liver disease. Appropriate parenteral nutrition formulation, delivery, and close monitoring markedly decrease the risks associated with parenteral nutrition.
The choice of nutrition administered (oral, enteral and parenteral nutrition) is dictated by the baby’s health condition and level of maturity.
Please keep in mind that enteral nutrition should be advanced as rapidly as tolerated and should increasingly replace parenteral nutrition. When both, enteral and parenteral nutrition are considered, enteral nutrition should always be prioritised.
A warm thank you goes out to Prof. Dr. Berthold Koletzko for his great advice and help on this website content.
The content was last reviewed in February 2018
For further information download our Factsheet and Position paper on parenteral nutrition.